Most conversations about menopause focus on one thing: that you have less estrogen than you used to. And that is true. But there is a deeper, less-discussed story that may explain why some women struggle through this transition far more than others — and why two women with similar hormone levels on a blood test can feel completely different.
The real question is not just how much estrogen you have. It is what kind.
Meet Your Two Estrogens
Your body produces several types of estrogen, but two are central to this conversation.
The estrogen your ovaries made throughout your reproductive years. The full-strength, premium version — the one that protected your bones, kept your brain sharp, stabilized your mood, regulated your body temperature, and supported deep, restorative sleep.
Think of it as the original document: clear, precise, and fully functional.
A weaker, less stable form of estrogen. Still present in the body, but carrying only a fraction of estradiol's protective power. Produced primarily by fat tissue, not the ovaries.
Think of it as a photocopy of the original: recognizable, but lacking the clarity and strength of the source.
During your reproductive years, estradiol dominated. After menopause, as the ovaries step back from hormone production, the balance shifts. Research published in peer-reviewed endocrinology journals confirms that estrone becomes the dominant estrogen in postmenopausal women, produced primarily by fat tissue rather than the ovaries. This shift is normal and expected. But how far the balance tips — and how your body uses what it has — depends on factors that are very much within your influence.
Where Does Testosterone Fit In?
You may be surprised to learn that testosterone plays a key role in estrogen production — in women as well as men. After menopause, one of the body's main strategies for producing estrogen is to convert testosterone into it. Your body uses a conversion process — think of it like a chemical translation — to turn testosterone into estrogen.
But here is where it gets important: the type of estrogen that results from this conversion is not fixed. It depends on where in the body the conversion happens, and what conditions are present at the time.
When conversion happens in healthy, low-inflammation tissues — the brain, muscle, skin, and blood vessels — the result tends to be estradiol, the premium version. When conversion happens in fat tissue — particularly the belly fat that tends to accumulate after menopause — or in inflamed tissues, the result tends to be estrone, the weaker photocopy.
Your body is constantly making choices about where and how to convert testosterone. And those choices are heavily influenced by one factor that most women never connect to their hormones: stress.
How Stress Changes Your Hormone Chemistry
Think of your body's hormonal system as a production facility with limited resources. When everything is running calmly and efficiently, the facility produces high-quality output — in this case, estradiol — delivered to where it is needed most.
When chronic stress enters the picture, the facility gets a new priority directive: make cortisol. Cortisol is your stress-response hormone — it exists to mobilize your body for danger. The problem is that cortisol and your sex hormones are made from the same raw materials. When your body is under sustained stress, those raw materials get redirected toward cortisol production at the expense of your sex hormones, including progesterone.
Progesterone, which normally helps balance estrogen's effects in the body, gets depleted. The hormonal environment shifts. And as this happens, the conversion of testosterone into estrogen begins to favor the wrong pathway — not toward estradiol in the brain and muscle, but toward estrone in fat tissue and inflamed areas.
The result is what researchers describe as estrone dominance: a state where your body has estrogen-level activity — enough to trigger estrogen-related symptoms — but not the stable, protective estradiol that your body actually needs.
You may experience hot flashes, anxiety, mood instability, and brain fog not because you have no estrogen, but because you have the wrong kind, delivered inconsistently, without the steadying effect of estradiol.
Research has confirmed this connection. Chronic stress elevates cortisol, which disrupts the hormonal pathways that favor estradiol production. Fat tissue — especially the visceral belly fat that grows with stress and menopause — preferentially produces estrone. Inflammation, which stress drives and estradiol normally helps control, further tips the balance in the wrong direction.
There is also a vicious cycle at work. Estradiol itself helps your body manage the stress response. When estradiol declines, your system becomes more reactive to stress. More stress means more cortisol. More cortisol means further disruption of estradiol production. The spiral continues.
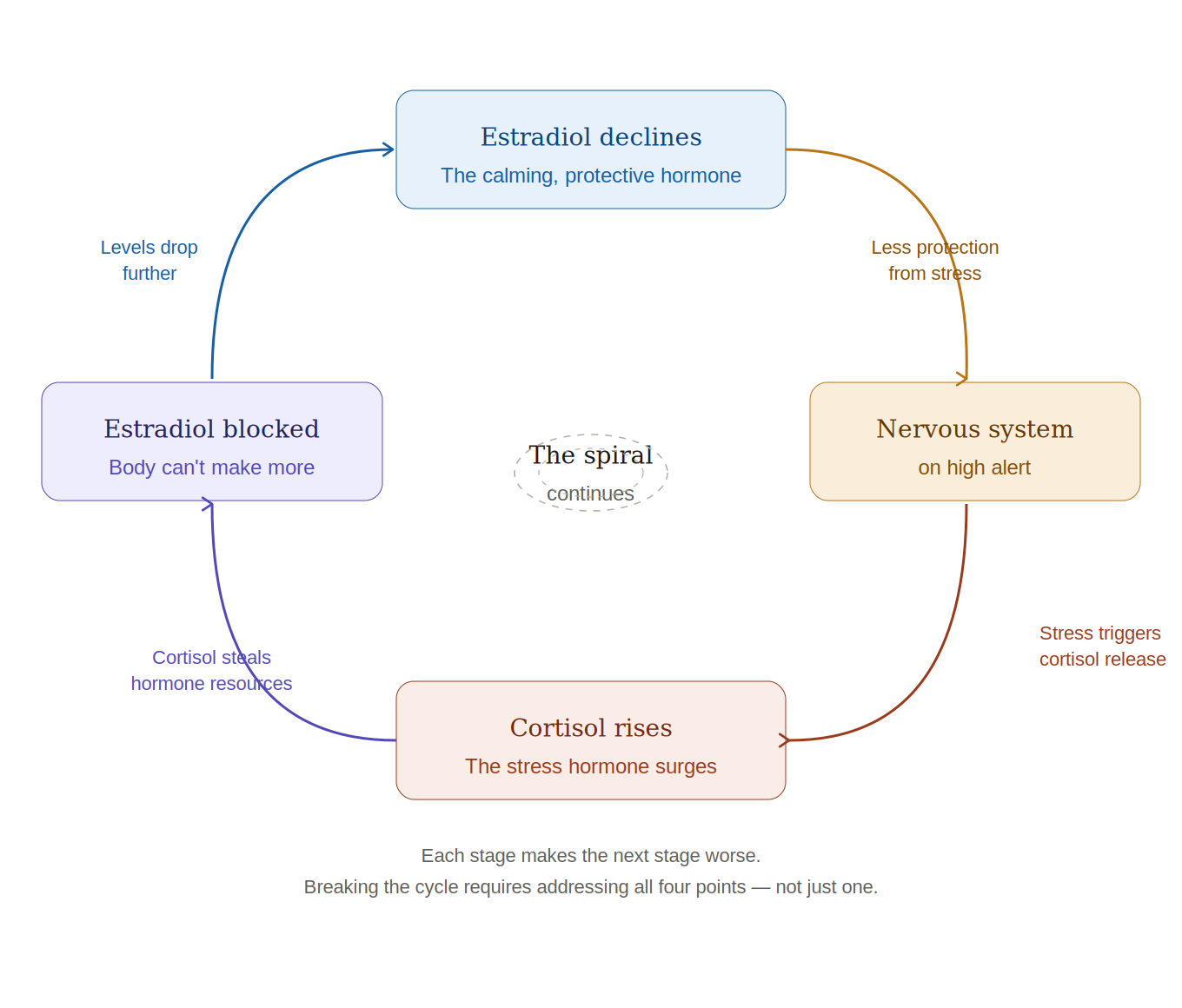
Each stage makes the next stage worse. Breaking the cycle requires addressing all four points — not just one.
Why This Matters — and What You Can Do
Understanding this changes how you think about menopause and what you can actually do about it.
It means that the difference between a smooth transition and a difficult one is not simply determined by your age or your genes. It is significantly shaped by the state of your stress system, your inflammation levels, the health of your liver and gut, the amount of belly fat you carry, and the quality of your sleep.
Every strategy that reduces chronic stress — genuine rest, movement, nutrition that keeps blood sugar stable, time in nature, and most importantly, strengthening the spiritual connection in order to address unresolved emotional weight and fear — is also a hormonal intervention.
A woman who enters menopause carrying years of unresolved stress, with elevated inflammation, unhealthy gut, and disrupted sleep, is not just emotionally depleted — her hormone conversion machinery is working against her. A woman who has tended to her inner world, her nervous system, and her physical health is giving her body the conditions it needs to produce and use the better form of estrogen, even in the absence of the ovaries.
A Word from The Healing Dawn
This is precisely why, at The Healing Dawn, we never look at hormones in isolation. Your hormone profile is not just a number on a lab result — it is a reflection of how your whole system is functioning. Your stress history, your gut health, the burden your liver carries, the quality of your rest, and the state of your spirit all shape what your body does with the hormones it has.
When we work with women navigating this transition, we are not simply trying to replace what the ovaries have stopped producing. We are working to restore the conditions under which your body can produce, convert, and use its hormones wisely — and to address the deeper sources of dysregulation that no supplement alone can reach.
The goal is not just hormonal balance. It is the kind of whole-person restoration that makes that balance possible and lasting.
It is not just how much estrogen you have — it is what kind.
Stress changes the quality of your hormone chemistry, not just the quantity.
Tending to your nervous system, your inner world, and your physical health is not separate from hormonal health. It IS hormonal health.